
 Download PDF
Download PDF Download PDF
Download PDFMarket Overview
The USA predictive analytics in healthcare market is valued at USD ~ billion in 2024 and USD ~ billion in 2024, as tracked by a U.S.-specific market sizing series. Growth is being pushed by the operationalization of advanced analytics on top of expanding EHR and claims datasets, payer demands for risk scoring and fraud/waste detection, and provider focus on readmission prevention and capacity optimization. The market is also being reinforced by enterprise-scale AI/ML deployments that embed predictive models into clinical workflow, revenue-cycle, and population health programs.
Within the USA, adoption is concentrated in major health-tech and payer/provider hubs such as the San Francisco Bay Area (AI and cloud ecosystem), Boston–Cambridge (academic medical centers and life sciences data), New York City (payer headquarters and large IDNs), Chicago (health system networks and analytics services), and Nashville (healthcare services and hospital operator density). These hubs dominate due to deeper data infrastructure, larger integrated delivery networks, higher density of analytics vendors and health IT talent, and earlier migration to cloud/enterprise platforms that can support model lifecycle management and governance at scale.
Market Segmentation
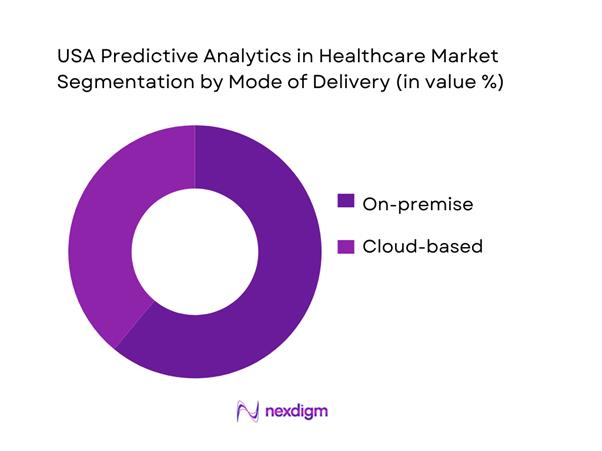
By Mode of Delivery
The USA Predictive Analytics in Healthcare market is segmented into on-premise and cloud-based deployments. On-premise deployments hold the dominant share because many large U.S. health systems built their analytics stacks around legacy data warehouses, on-site integration engines, and local security controls for protected health information. In acute-care environments, on-premise architectures also support lower-latency inference for workflow-sensitive use cases such as deterioration alerts, sepsis risk scoring, bed-flow prediction, and operating-room throughput optimization. Another driver is governance: institutions often prefer direct control over access logging, model monitoring, and audit readiness—especially when predictive outputs affect clinical decisions, reimbursement integrity, or utilization management. While cloud adoption is accelerating for scalable training and multi-site aggregation, on-premise remains entrenched where modernization cycles are long and data-migration risk is high.
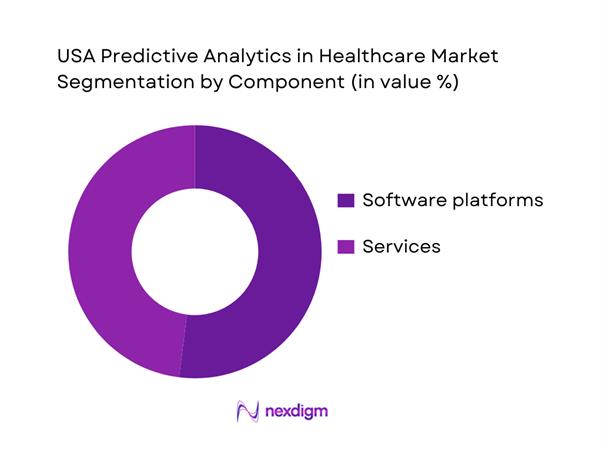
By Component
The USA Predictive Analytics in Healthcare market is segmented into software platforms and services. Software platforms lead because U.S. buyers increasingly standardize on enterprise analytics layers that can be reused across multiple workflows—clinical risk stratification, payer claims integrity, denial prediction, care-gap closure, and operational command centers—rather than funding disconnected point solutions. Platform adoption is also supported by the need for repeatable model lifecycle management (data pipelines, feature stores, validation, monitoring, and governance) across many hospitals and service lines. Vendors that bundle predictive models inside EHR/RCM/population health modules reduce time-to-value and improve clinician adoption by integrating alerts into existing workflows. Services remain sizable because deployments require interoperability work, data normalization, change management, and continuous model tuning; however, the spend is increasingly anchored by recurring platform subscriptions with services layered on top.
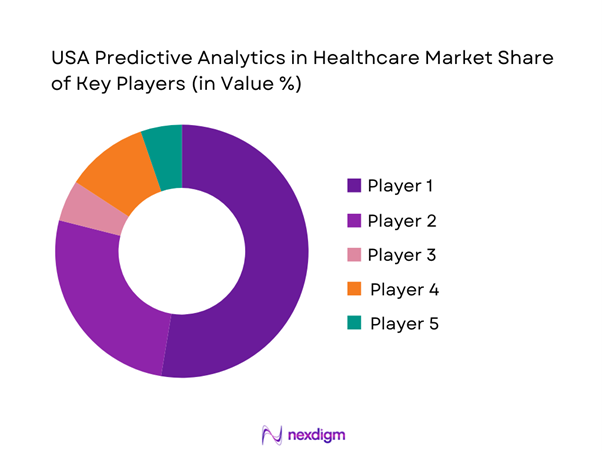
Competitive Landscape
The USA predictive analytics in healthcare market is moderately consolidated around EHR-native analytics stacks, payer analytics platforms, and enterprise data/AI vendors, with specialist healthcare analytics firms competing on faster implementation, domain models, and managed-service delivery. Competitive differentiation is increasingly defined by (i) depth of clinical workflow integration, (ii) interoperability readiness, (iii) model governance/monitoring, and (iv) scalability across multi-hospital systems and payer networks.
| Company | Est. Year | HQ | Core Healthcare Predictive Analytics Strength | Primary Buyer Focus | Deployment Preference | Interoperability & Data Sources | Differentiation / Go-to-Market (U.S.) |
| Epic Systems | 1979 | USA | ~ | ~ | ~ | ~ | ~ |
| Oracle Health (Cerner) | 1979 | USA | ~ | ~ | ~ | ~ | ~ |
| Optum (UnitedHealth Group) | 2011 | USA | ~ | ~ | ~ | ~ | ~ |
| SAS | 1976 | USA | ~ | ~ | ~ | ~ | ~ |
| IBM | 1911 | USA | ~ | ~ | ~ | ~ | ~ |
USA Predictive Analytics in Healthcare Market Analysis
Growth Drivers
Value-Based Care and Risk-Bearing Expansion
The USA’s shift toward accountability-based reimbursement is structurally increasing demand for predictive risk stratification, attribution, and total-cost-of-care forecasting inside payer and provider workflows. As of the latest reported performance cycle, the Medicare Shared Savings Program had ~ ACOs with ~ assigned beneficiaries, creating a large, continuously refreshed pool of claims + clinical utilization signals that health systems use for prospective risk scoring, care-gap prediction, and avoidable utilization prevention. Predictive analytics becomes a “core operating layer” in ACOs because benchmarks, quality scoring, and savings calculations require longitudinal modeling across episodes. At the macro level, the USA’s economy (GDP) is USD ~ trillion with GDP per capita USD ~, supporting sustained employer-sponsored coverage scale and large administrative datasets that make actuarial-style prediction feasible. These risk-bearing structures also amplify the need for explainable models, member-level documentation trails, and auditable patient cohort logic that can survive compliance reviews without relying on manual spreadsheets.
Capacity Optimization and Throughput Pressures
Throughput constraints across emergency, inpatient, and post-acute pathways are a major driver because predictive analytics directly targets bottlenecks (admissions prediction, length-of-stay prediction, discharge readiness, ICU step-down probability, staffing optimization). In the USA, emergency departments recorded ~ visits and ~ ED visits resulting in hospital admission, reflecting the scale of operational variability that predictive models are designed to smooth—especially when hospitals face bed-management and boarding pressures. Separately, national inpatient utilization datasets used for benchmarking estimate over ~ hospitalizations annually, indicating why real-time forecasting is increasingly operationalized in command centers. These workloads sit inside an economy of USD ~ GDP, where hospital systems’ productivity expectations and labor scarcity pressures increase adoption of automated forecasting and early-warning tools. Predictive analytics is favored because it converts daily operational data into probabilistic schedules (beds, OR time, imaging slots) and prioritization rules that reduce avoidable delays without expanding physical capacity.
Challenges
Data Quality and Coding Variability
Predictive models are only as reliable as the upstream data, and U.S. healthcare data quality is constrained by inconsistent coding practices, documentation variation across provider groups, and shifting payer edits that create “label noise” in claims. Program integrity statistics illustrate the magnitude of documentation/coding risk: CMS estimated USD ~ billion in Medicare Fee-for-Service improper payments, where a large portion of errors typically relate to insufficient documentation or coding issues rather than intentional fraud—exactly the kind of variability that can mislead model training and degrade inference stability if not governed. In clinical settings, chronic disease coding and comorbidity capture also varies across EHR workflows, affecting risk scores and cohort definitions. This challenge is structural because the U.S. system processes spending at USD ~ trillion scale and relies on massive code-based transactions, increasing the probability of inconsistent capture. Even with a GDP of USD ~ trillion, organizations still face heavy operational effort in standardizing terminologies, cleaning encounter data, and validating labels before deploying predictive models into decision pathways that affect care or payment.
Interoperability and Patient Identity Resolution
Even with better exchange, matching records across organizations remains difficult due to incomplete demographics, inconsistent identifiers, and fragmented patient history across payer/provider networks. Patient identity resolution becomes a hard constraint when predictive models require longitudinal event sequences (ED visits, admissions, pharmacy fills) from multiple sources—small mismatch rates can generate large modeling errors at population scale. The operational environment intensifies this: the USA has ~ ED visits and ~ ED-to-admission events, creating huge volumes of high-frequency transitions where identity mismatches and incomplete outside-history reduce model signal quality right at the point of care. Governance and trust frameworks like TEFCA are intended to support standardized exchange, but operationalizing exchange still requires robust matching logic, reconciliation workflows, and auditability—especially when clinical predictions could trigger interventions. The macro context (GDP USD ~ trillion) supports investment, yet fragmentation across thousands of entities makes uniform identity practices slow to implement. As a result, many deployments remain limited to “within-system” predictions or require expensive data normalization layers before models can generalize across networks.
Opportunities
AI-Augmented Care Management
The most scalable opportunity is expanding predictive analytics from “risk scores” to AI-augmented care management that prioritizes outreach, closes care gaps, and reduces avoidable utilization—without relying on future projections. The U.S. chronic burden provides immediate runway: estimates indicate ~ people have at least one major chronic disease and ~ people have diabetes, creating large cohorts where predictive targeting can improve program efficiency (who to call, who needs medication support, who is likely to deteriorate). In value-based arrangements, the MSSP footprint alone includes ~ assigned beneficiaries, providing continuous learning data for model refinement and operational playbooks at scale. The opportunity strengthens as interoperability frameworks mature and as AI-enabled tools expand inside regulated ecosystems, increasing organizational comfort with AI governance. With GDP USD ~ trillion, large employers and health plans can fund longitudinal care programs, and predictive analytics becomes the coordination layer that allocates finite care manager time to the highest-impact members—improving outcomes while reducing preventable ED use and admissions.
Predictive Revenue Cycle and Denials Prevention
A high-ROI opportunity is predictive analytics embedded in revenue cycle operations—preventing denials, reducing documentation errors, and improving coding accuracy using current program integrity signals (without referencing market size or pricing). CMS estimated USD ~ billion in Medicare Fee-for-Service improper payments, and Medicare Part C improper payments of USD ~ billion, illustrating how documentation gaps, coding issues, and administrative errors create direct financial leakage and post-payment risk. Predictive tools can prioritize charts likely to fail medical necessity checks, flag missing documentation before claim submission, and identify patterns associated with recoupment risk—reducing rework and protecting cash flow. This opportunity is especially relevant at system scale given U.S. health expenditures of USD ~ trillion and the sheer volume of hospital and physician claims generated by ~ ED visits and tens of millions of hospitalizations. With GDP USD ~ trillion, organizations can justify enterprise-grade analytics because even small reductions in avoidable denials and rework translate into significant operational savings and compliance resilience—especially when audits and payer edits become more stringent.
Future Outlook
Over the next planning cycle, the USA Predictive Analytics in Healthcare market is expected to expand as providers and payers industrialize AI/ML across clinical, financial, and operational workflows—moving from pilots to governed, scaled deployments. Growth will be sustained by EHR data expansion, payer pressure for measurable outcomes and cost control, and the rise of platform-based analytics that standardize model monitoring and compliance. The fastest traction is expected where predictive models directly reduce avoidable utilization, improve throughput, strengthen reimbursement integrity, and support population-risk programs at enterprise scale.
Major Players
- IBM
- Oracle Health
- Epic Systems
- Optum
- SAS
- McKesson
- Microsoft
- Siemens Healthineers
- GE HealthCare
- Health Catalyst
- MedeAnalytics
- Inovalon
- Allscripts
- Welltok
Key Target Audience
- Hospital systems and Integrated Delivery Networks
- Health insurance payers & managed care organizations
- Accountable Care Organizations (ACOs) and risk-bearing provider groups
- Pharmacy Benefit Managers (PBMs) and specialty care managers
- Healthcare IT and digital transformation leadership
- Medical device, RPM, and digital therapeutics firms
- Investments and venture capitalist firms
- Government and regulatory bodies
Research Methodology
Step 1: Identification of Key Variables
We begin by building a U.S. ecosystem map covering providers, payers, EHR vendors, analytics platform vendors, and managed-service integrators. We define market boundaries (predictive analytics used for clinical, financial, and operational healthcare decisions) and lock assumptions on revenue recognition across software and services.
Step 2: Market Analysis and Construction
We compile historical and current pricing/revenue signals from vendor disclosures, healthcare IT spend indicators, and published market sizing series. The objective is to construct a reconciled view of demand across payer, provider, and hybrid buyers, adjusting for multi-year contract structures and implementation-led revenues.
Step 3: Hypothesis Validation and Expert Consultation
We validate adoption and spend hypotheses through expert consultations (CATI-style) with healthcare CIO/CDO teams, payer analytics leaders, and implementation partners. These discussions are used to confirm deployment patterns, dominant use cases, procurement cycles, and model governance requirements.
Step 4: Research Synthesis and Final Output
We triangulate top-down market signals with bottom-up workflow adoption (EHR analytics modules, RCM analytics, population health platforms, and payer risk tools). We then finalize the market model, segmentation benchmarks, and competitive positioning with consistency checks across data sources.
- Executive Summary
- Research Methodology (Market Definitions and Assumptions, Abbreviations, Predictive Analytics Value-Chain Boundary, Market Sizing Approach, Triangulation Logic, Primary Interview Mix by Stakeholder Type, Data Validation and Model-Readiness Scoring, Limitations and Future Conclusions)
- Definition and Scope
- Market Evolution and Genesis
- Timeline of Major Technology and Policy Milestones
- Healthcare Business Cycle Touchpoints
- Data Supply Chain and Value Chain
- Typical Predictive Workflows and Output Formats

- Growth Drivers
Value-Based Care and Risk-Bearing Expansion
Capacity Optimization and Throughput Pressures
Chronic Disease Burden and Care Complexity
Payer Cost Containment and Medical Management
Interoperability Progress and Data Availability - Challenges
Data Quality and Coding Variability
Interoperability and Patient Identity Resolution
Algorithm Governance and Clinical Safety
Workflow Integration and Adoption Barriers
Procurement, Security, and Compliance Reviews - Opportunities
AI-Augmented Care Management
Predictive Revenue Cycle and Denials Prevention
Imaging and Pathology Predictive Analytics
Social Determinants of Health Integrated Risk Models
Federated Learning and Privacy-Preserving Analytics - Trends
Shift Toward Platform and Marketplace Models
Transition from Insights to Automated Interventions
Real-Time and Near-Real-Time Risk Scoring
Explainability and Transparency by Design
Convergence of Predictive Analytics with Generative AI - Regulatory & Policy Landscape
- SWOT Analysis
- Stakeholder & Ecosystem Analysis
- Porter’s Five Forces Analysis
- Competitive Intensity & Ecosystem Mapping
- By Value, 2019–2024
- By Volume, 2019–2024
- By Average Contract Value, 2019–2024
- By End-Use Industry (in Value %)
Providers
Payers
Life Sciences
Public Health and Government Programs
Employers and Benefit Managers - By Application (in Value %)
Inpatient and Acute Care
Outpatient and Ambulatory Care
Emergency and Urgent Care
Home Health and Post-Acute Care
Pharmacy and Specialty Pharmacy - By Technology Architecture (in Value %)
Readmission and Length-of-Stay Forecasting
Clinical Deterioration and Sepsis Prediction
Chronic Disease Risk Stratification
Population Health and Preventive Screening
Utilization and Cost of Care Prediction
Claims Integrity and Payment Accuracy - By Connectivity Type (in Value %)
EHR Data Feeds
Claims Data Pipelines
Lab and Imaging Data
Social Determinants of Health Data
Device, Remote Monitoring, and Wearables Data - By Region (in Value %)
Northeast
Midwest
South
West
- Market Share Assessment
Share by End User Cluster
Share by Primary Use Case - Cross Comparison Parameters (EHR-native integration depth, FHIR and TEFCA interoperability readiness, model governance and drift monitoring tooling, real-time scoring latency and service-level commitments, data-source breadth across clinical and non-clinical datasets, clinical workflow embedment depth, privacy and de-identification architecture, value realization and ROI measurement toolkits)
- SWOT Analysis of Major Players
- Pricing and Packaging Analysis
- Detailed Profiles of Major Companies
Epic Systems
Oracle Health
Optum Insight
Health Catalyst
Innovaccer
SAS
IBM
Microsoft
Google Cloud
Amazon Web Services
Palantir
Databricks
Snowflake
Arcadia
Cotiviti
- Demand and Utilization Patterns
- Budget Ownership and Buying Centers
- Evaluation Criteria and Vendor Selection
- Needs, Desires, and Pain Point Analysis
- Decision-Making Process
- By Value, 2025–2030
- By Volume, 2025–2030
- By Average Contract Value, 2025–2030




 Request a Sample
Request a Sample Ask for Customization
Ask for Customization Get a Quote
Get a Quote Enquire Now
Enquire Now